Interesting Day
Saw some interesting cases today. The morning was full of normal stuff, like colonoscopies and gastroscopies - with little more to find than polyps and ulcers. That stuff is kind of boring - its the same thing all the time. But in the afternoon, things picked up a little. There were two patients, both with alcoholic liver disease, both presenting with haematemesis and malaena.
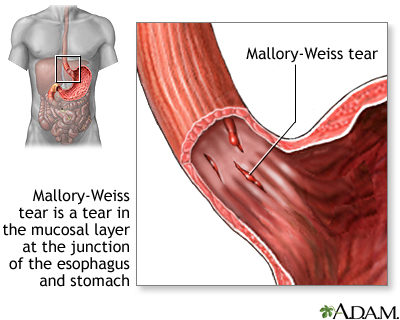
The first guy was an IV drug user (he shot up on speed). He came in with a history of vomiting up blood for the last few days, and was rushed to the endoscopy suite from ED. Anyway, when we went in there was blood everywhere. It was difficult to see anything else really. We looked around the stomach and duodenum, ascertained that it was all normal, and then went back to the oesophagus to see where the blood was coming from. There were two longitudinal tears in the mucosa which were obviously the source of the bleeding. So we looked at them, and then the consultant suggested injecting them with adrenaline, which they did. And the bleeding gradually stopped: a) because of the mass effect of the adrenaline blebs, and b) because of the vasoconstrictive effect of the adrenaline. It turned out that they were both Mallory-Weiss tears. John told me about something else I hadn't heard before, Boerhaave's Syndrome, a complication of an oesophageal tear in which there is a pneumomediastinum. Diagnosis is by CT.

The second patient was pretty interesting. He was completely off his face, hepatic encephalopathy in full effect. He was totally disoriented, didn't know anything about his surroundings. On top of that, he was Hep C positive and had massive ascites. He had to be scoped on his back, with lots of us restraining him! Anyway, we went in and saw nothing much really - there were a few varices but they weren't bleeding (most likely due to the fact that his fluid had all shifted into his ascites). Then we saw a small tear in one of them. That was it! Out came the bands (variceal bands, duh) (which I hadn't seen before). Anyway, that was cool. They suck up the varices into a port which they attached to the end of the scope. There's a wire that runs from that port to the control trigger in the operator's left hand. So as they suck up the varix, the scoper releases the cord, and a little blue rubber band is released and gets stuck on the varix! Problem solvered. It was great!
The first guy was an IV drug user (he shot up on speed). He came in with a history of vomiting up blood for the last few days, and was rushed to the endoscopy suite from ED. Anyway, when we went in there was blood everywhere. It was difficult to see anything else really. We looked around the stomach and duodenum, ascertained that it was all normal, and then went back to the oesophagus to see where the blood was coming from. There were two longitudinal tears in the mucosa which were obviously the source of the bleeding. So we looked at them, and then the consultant suggested injecting them with adrenaline, which they did. And the bleeding gradually stopped: a) because of the mass effect of the adrenaline blebs, and b) because of the vasoconstrictive effect of the adrenaline. It turned out that they were both Mallory-Weiss tears. John told me about something else I hadn't heard before, Boerhaave's Syndrome, a complication of an oesophageal tear in which there is a pneumomediastinum. Diagnosis is by CT.
The second patient was pretty interesting. He was completely off his face, hepatic encephalopathy in full effect. He was totally disoriented, didn't know anything about his surroundings. On top of that, he was Hep C positive and had massive ascites. He had to be scoped on his back, with lots of us restraining him! Anyway, we went in and saw nothing much really - there were a few varices but they weren't bleeding (most likely due to the fact that his fluid had all shifted into his ascites). Then we saw a small tear in one of them. That was it! Out came the bands (variceal bands, duh) (which I hadn't seen before). Anyway, that was cool. They suck up the varices into a port which they attached to the end of the scope. There's a wire that runs from that port to the control trigger in the operator's left hand. So as they suck up the varix, the scoper releases the cord, and a little blue rubber band is released and gets stuck on the varix! Problem solvered. It was great!





{kind=link}
{kind=link}
{kind=link}
0 Comments:
Post a Comment
<< Home